LETTER TO THE EDITOR |
https://doi.org/10.5005/jp-journals-10028-1609 |
Continuous End-tidal CO2 Monitoring during Awake Craniotomy: A Reliable Makeshift Modality
1-4Department of Anesthesiology and Intensive Care, Postgraduate Institute of Education and Research (PGIMER), Chandigarh, India
Corresponding Author: Rajeev Chauhan, Department of Anesthesiology and Intensive Care, Postgraduate Institute of Education and Research (PGIMER), Chandigarh, India, Phone: +91 7087422950, e-mail: dr.rajeevchauhan@gmail.com
Received on: 25 May 2022; Accepted on: 13 June 2022; Published on: 31 December 2022
How to cite this article: Singh N, Sarna R, Chauhan R et al. Continuous End-tidal CO2 Monitoring during Awake Craniotomy: A Reliable Makeshift Modality. J Postgrad Med Edu Res 2022;56(4):197-198.
Source of support: Nil
Conflict of interest: None
Awake craniotomy to remove intra-axial tumors within or adjacent to eloquent brain regions requires an awake and cooperative patient for immediate neurological testing. Fluctuations in the sedation level may lead to airway obstruction and consequent hypercapnia, hypoxia, increased intracranial pressure with a “tight” brain, or conversely, an inadequately sedated, anxious, and uncomfortable patient.1 The key components of monitoring include the continuous communication with the patient along with observation of oxygenation, circulation, temperature, and watching for local anesthesia toxicity. Respiratory rate and clinical observation provide a clue regarding the ventilation, albeit direct visualization of chest movement and immediate access to the patient’s airway remains a limitation.
Capnography is a real-time monitoring component that allows dynamic assessment of the ventilatory status and any impending apnea at the earliest.2 However, in spontaneously breathing patients, the carbon dioxide (CO2) levels are often inaccurate. Although a pulse oximeter is a reliable tool to monitor oxygenation, a drop-in saturation lags behind hypoventilation, more so if the patient is receiving supplemental oxygen. Moreover, it has been demonstrated that continuous capnometry identifies airway obstruction, apnea, or hypoventilation prior to both clinical detections of airway issues or the development of hypoxia.3 Use of capnography in nonintubated patients is challenging and inaccurate because of dilution of expired gas with varying oxygen flows, mask design, issues with the sampling line, etc.4 An inadequate sampling of alveolar air, mixing of inspired and expired gases, and air leaks are the problem associated with the use of nasal sampling devices in spontaneously breathing patients.5 Availability of special capnography masks, and devices is a challenge in a resource-poor country like ours. We developed a low-cost, effective method with commonly available tools in operation theater to continuously monitor end-tidal CO2 (EtCO2) in a spontaneously breathing patient undergoing awake craniotomy.
The patient, in this case, was operated on for a tumor on the motor strip in the lateral position. Monitors were attached, and dexmedetomidine loading and fentanyl infusion were started. After adequate sedation, a scalp block was given, and a 7 mm internal diameter nasopharyngeal airway was inserted. We attached a T-piece, which was connected to oxygen tubing on one side, and a three-way with 10 cm on another side to the nasopharyngeal airway. The EtCO2 sampling line was attached to the other port of the three-way with 10 cm (Fig. 1A).
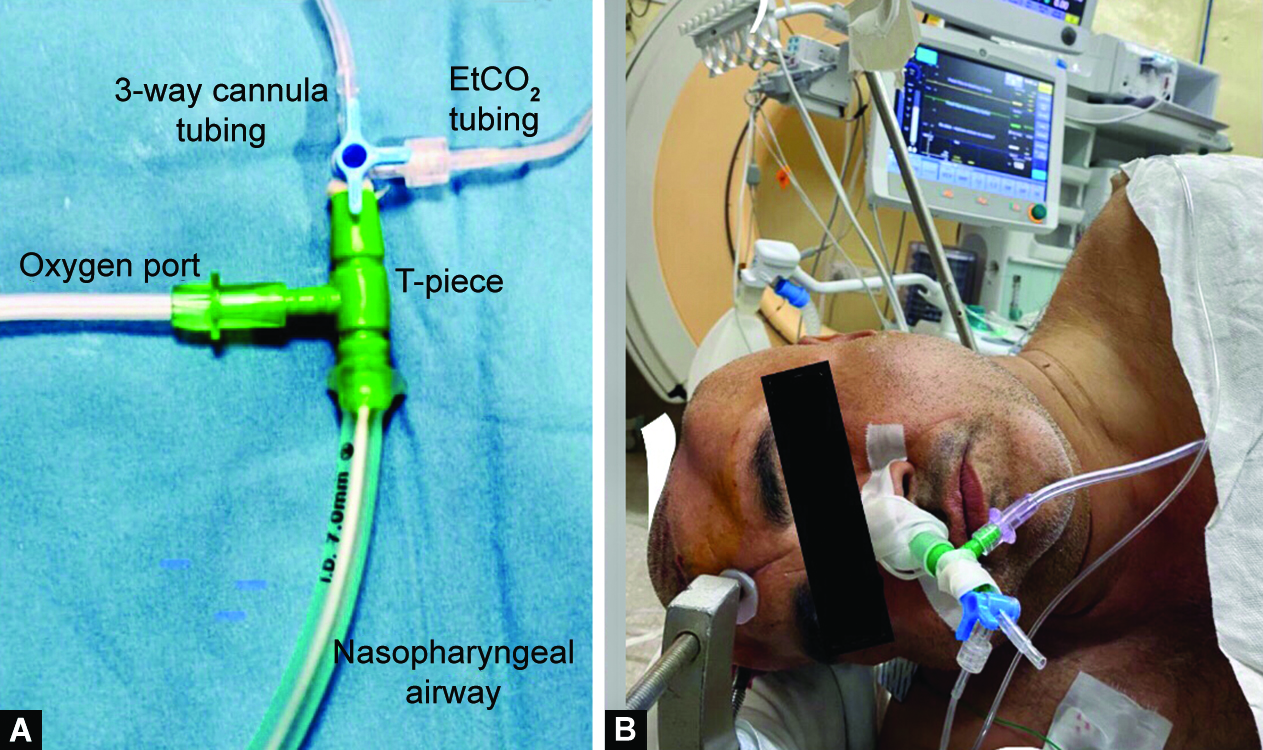
Figs 1A and B: (A) Assembly for monitoring EtCO2; (B) Patient with the assembly
The assembly comprising the nasopharyngeal airway, T-piece, and the three-way with 10 cm with the EtCO2 sampling line gave us a continuous capnography EtCO2 recording. The values of EtCO2 (average 32 mm Hg) were comparable with the partial pressure of CO2 values of the five arterial blood gas samples (31 mm Hg) taken during the procedure. However, one may raise concerns regarding the bulkiness of the above assembly, but in our case (Fig. 1B), the patient tolerated the 3-hour procedure well without any discomfort. This modality provides an easy, cost-effective, and near-accurate way to monitor EtCO2 in spontaneously breathing patients.
REFERENCES
1. Kim SH, Choi SH. Anesthetic considerations for awake craniotomy. Anesth Pain Med (Seoul) 2020;15(3):269–274. DOI: 10.17085/apm.20050
2. Manifold CA, Davids N, Villers LC, et al. Capnography for the nonintubated patient in the emergency setting. J Emerg Med 2013;45(4):626–632. DOI: 10.1016/j.jemermed.2013.05.012
3. Burton JH, Harrah JD, Germann CA, et al. Does end-tidal carbon dioxide monitoring detect respiratory events prior to current sedation monitoring practices? Acad Emerg Med 2006;13(5):500–504. DOI: 10.1197/j.aem.2005.12.017
4. Phillips JS, Pangilinan LP, Mangalindan ER, et al. A comparison of different techniques for interfacing capnography with adult and pediatric supplemental oxygen masks. Respir Care 2017;62(1):78–85. DOI: 10.4187/respcare.05111
5. Fitzpatrick LJ. The Correlation Between End-Tidal Carbon Dioxide Measured by Capnoxygen (Trade Mark) Mask and Nasal Cannula. Uniformed services Univ of the health sciences Bethesda MD; 2000 Oct 1.
________________________
© The Author(s). 2022 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.